Dear Community members, We are reaching out to ask for your support in sharing a first of several survey ‘s...
Prevention and Management of Urinary Tract Infections
By Kelly TennantWhat is a urinary tract infection?
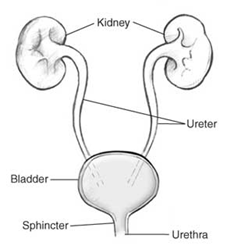
Commonly referred to as a UTI, a urinary tract infection is an overgrowth of bacteria occurring at any point in the urinary tract. They are also sometimes called bladder infections or kidney infections. A lower UTI affects the urethra or bladder while an upper UTI affects the ureters or kidneys.
Why are people with SCI at risk of UTIs?
Anyone can get a UTI, but people with spinal cord injuries are more susceptible than the general population. It is estimated that the typical person with SCI will experience 2.5 UTIs per year. Your individual risk will vary depending on your ability to fully empty your bladder, whether or not you catheterize, and how well your body fights infections.
Virtually all individuals with spinal cord injuries have a condition called neurogenic bladder, where the SCI impacts the ability of the bladder to store or void urine. Reduced bladder function leads to urinary stasis (leftover urine staying in the bladder after emptying, also called post-void residuals or PVRs). High PVRs promote the growth of bacteria in the bladder.
Using a catheter for bladder management, whether that is intermittent (straight cathing) or indwelling (Foley or suprapubic), increases the risk of UTIs because bacteria can be pushed into the urethra and bladder with the catheter.
How do I know if I have a UTI?
Symptoms of a UTI will depend on your level of sensation and the severity of the infection. If you have very limited sensation, you may not realize you have a UTI until it is already very severe.
You may have a UTI if you are experiencing one or more of the following symptoms:
| Pain with urination | Increased muscle spasms |
| Increased frequency or urgency | Feeling tired or sluggish |
| Leaking urine | Fever over 38°C |
| Dark, cloudy or blood-tinged urine | Chills |
| Foul smelling urine | Nausea |
| Urine with mucus or sediment | Headache |
| Lower abdominal or lower back pain | Autonomic dysreflexia (injuries T6 or higher) |
What should I do if I suspect I have a UTI?
Call you family doctor at the first signs of a UTI and try to get a same-day appointment. If you are not able to get in with your regular doctor, go to the nearest walk-in clinic or urgent care centre. It is important to start antibiotic treatment as soon as an infection is confirmed as UTIs can very quickly become serious.
Important note: It is usually not necessary to go to the emergency room for a UTI unless you are experiencing symptoms of sepsis (very high or very low temperature – over 38.3 or under 36, heart rate over 90 beats per minute, breathing rate over 20 breaths per minute, elevated blood sugar without diabetes, confusion or loss of consciousness, swelling of the extremities, neck or face, and decreased urine output). If you are experiencing symptoms of sepsis, call 911 immediately.

Your doctor will have you give a urine sample, which they will test with a dipstick right away, as well as generally send to a lab for a culture. The dipstick test confirms an infection, but doesn’t tell your doctor what is causing the infection. A culture will confirm the type of bacteria, but takes a couple of days to complete. You will likely leave with a prescription for a general antibiotic that tends to work well for UTIs, but if the culture results show that a different antibiotic would be better for fighting the specific type of bacteria, your doctor may call you with the results and a new prescription. If your symptoms are mild, your doctor may wait to prescribe an antibiotic until the culture results come back, and encourage you to drink more water to try to flush out the bacteria on your own. In this case, it is important to let your doctor know if your symptoms get worse.
If you are still having symptoms of the UTI after finishing the course of antibiotics or if symptoms disappear and then reappear a week or two later, contact your doctor, as you may need to try another antibiotic to completely get rid of the infection. Don’t stop taking the antibiotic once you start feeling better. It’s important to finish the full course of the prescription to prevent the infection from coming back. Very frequent urinary tract infections may be a sign of bladder or kidney stones, which form when the minerals in concentrated urine crystallize and clump together. Their jagged surface can be a hiding place for bacteria. Talk to your doctor if you suspect you have a stone, which is usually diagnosed via ultrasound imaging. Depending on the size, they may pass on their own, need to be “blasted” with a medical laser, or removed surgically.
What can I do to prevent UTIs?
Your best defense against UTIs is a combination of drinking plenty of water, emptying your bladder fully and frequently, and using clean technique for catheterization.
You can tell if you are drinking enough water by examining the colour of your urine. When you are well-hydrated, your urine should be clear or light yellow. If you are dehydrated, your urine will be dark yellow. This is a sign that you should be drinking more water to help flush out any bacteria that may be growing in your bladder. Aim for a total of 2 litres of water each day. Cut back or eliminate caffeine, alcohol, and sugary drinks, which contribute to dehydration.
Drinking more water will mean that your body will produce more urine. Try to empty your bladder completely at least every 4-6 hours, or more often if you are experiencing leakage or incontinence in between. If you use an indwelling catheter, you may need to empty your leg bag more often.
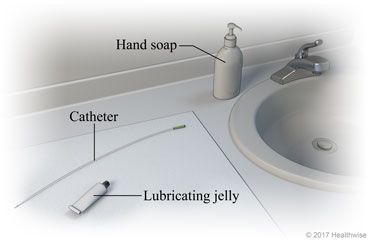
Use clean technique every time you catheterize. Make sure to wash your hands and the area around your urethral opening with water and a gentle soap. Many UTIs are caused by the bacteria naturally living on our skin being pushed into the bladder with the catheter. Women should wipe from front to back to avoid spreading bacteria from the anus. Avoid touching the insertable portion of the catheter, even with clean hands. Use only water-soluble lubricating jelly to lubricate your catheter before insertion. Take care to keep the tip and lid of your lube container clean to avoid contamination with bacteria, or use individual sterile packets. Never spit-lube or use petroleum-based lubricants; saliva contains bacteria and petroleum jelly may plug the catheter.
Single-use catheters are the best choice for reducing risk of infection, but if you cannot afford single-use catheters and must re-use your catheter, take the time to clean the catheter immediately after use with soap and water and allow it to air-dry completely by placing it in a clean towel or paper bag, which will allow for air flow. Consider investing in a supply of single-use catheters to use while away from home, where it can be harder to allow for proper air-drying.
If you use an indwelling catheter, make sure that clean technique is used during catheter changes, which should occur every 4 weeks. Change your catheter sooner if you have recently had a UTI or if the catheter becomes obstructed, hard, or changes colour.
What about cranberries?
This is one of the most common questions I get from clients concerned about UTIs. Unfortunately, there is conflicting evidence on the effectiveness of cranberry juice or concentrated cranberry tablets in the prevention and treatment of UTIs. Cranberry is thought to acidify urine, making it a less hospitable environment for bacterial growth as well as inhibiting the ability of bacteria to stick to the bladder wall. Although the research evidence is not conclusive, there is anecdotal evidence from many people that indicates individual benefits. Because of the risk of developing sepsis, using cranberry to treat a UTI instead of antibiotics is not recommended, but there is significantly less harm in trying to prevent UTIs with regular cranberry consumption. If it works for you, great! If not, keep trying other preventative measures.
One with a bit more scientific backing is D-Mannose. This is a naturally occurring sugar that is absorbed by the body much more slowly than glucose, so most of it ends up in our urine. Bacteria adhere to the D-Mannose molecules instead of the bladder walls, and are flushed out during urination. D-Mannose comes in powder form to be stirred into water and can be taken daily to help prevent UTIs or as a boost to antibiotic treatment to help treat a UTI.
Like all complementary or alternative treatments, it is best to speak with your doctor or pharmacist to ensure that any additional treatments will not interact negatively with your other prescriptions or medical conditions.
References
Garcia Leoni, M.E., & Esclarin De Ruz, A. (2003). Management of urinary tract infection in patients with spinal cord
injuries. Clinical Microbiology and Infection, 9, 780-785.
Goetz, L.L., Cardenas, D.D, Kennelly, M., Bonne Lee, B.S., Linsenmeyer, T., Moser, C., Pannek, J., Wyndaele, J.-J., &
Biering-Sorensen, F. (2013). International spinal cord injury urinary tract infection basic data set. Spinal Cord, 51, 700-704.
Model Systems Knowledge Translation Center. (2017, March). Urinary tract infection and spinal cord injury.
https://msktc.org/sites/default/files/SCI-UTI-508.pdf
Opperman, E.A. (2010). Cranberry is not effective for the prevention or treatment of urinary tract infections in
individuals with spinal cord injury. Spinal Cord, 48, 451-456.
Pannek, J. (2011). Treatment of urinary tract infection in persons with spinal cord injury: Guidelines, evidence, and
clinical practice. A questionnaire-based survey and review of the literature. The Journal of Spinal Cord Medicine, 34(1), 11-15.
Salameh, A., Mohajer, M.A., & Daroucihe, R.O. (2015). Prevention of urinary tract infections in patients with spinal
cord injury. Canadian Medical Association Journal, 187(11), 807-811.
Smith, J. & James, K. (2013). Eat well, live well with spinal cord injury. Paralyzed Veterans of America Education
Foundation.
University of Washington Department of Rehabilitation Medicine. (2020, February) SCI & urinary tract infections:
Intermittent catheterization. http://rehab.washington.edu/patientcare/patientinfo/articles/sci_uti.asp
Wagenlehner, F.M., & Pilatz, A. (2018) Preventing urinary tract infections in patients with neurogenic bladder. The
Lancet, 18(9), 926-927.